By clicking “Accept All Cookies”, you agree to the storing of cookies on your device to enhance site navigation, analyze site usage and assist in our marketing efforts.
By clicking “Accept All Cookies”, you agree to the storing of cookies on your device to enhance site navigation, analyze site usage and assist in our marketing efforts.
AI in Medical Device Complaint Processing
Why Intake Is Where Quality Fails Silently
Most quality teams invest in investigation tools, CAPA workflows, and regulatory reporting platforms. Almost none have solved the stage that precedes all of them — the fragmented, manual, language-heavy work of complaint intake. That is where timelines slip, signals disappear, and expertise gets wasted.
RandomTrees Editorial
Enterprise AI systems for regulated industries · Specialists in medical device quality operations, complaint management, and FDA/ISO-aligned AI deployment
7:42 AM, a hospital biomedical engineering department. A short email leaves a technician's inbox. A pump alarmed repeatedly during infusion. The unit was replaced. Please advise. No formal severity marker. No certainty the issue belongs to the device rather than maintenance, handling, or environment. It reads like routine correspondence — which is exactly the problem.By noon, customer support has forwarded it to a quality queue. Later that afternoon, a distributor in a separate market mentions similar behavior on a call — logged informally as a service note. Two days later, a field technician enters a related observation under a different product description in a different system. None of the three records are identical enough to trigger an automated keyword match. None individually forces urgency.Together, they may describe the earliest visible outline of a recurring safety issue. But in most organizations, they will not be connected for days — or at all.
Why Complaint Intake Fails Before Investigation Even Starts
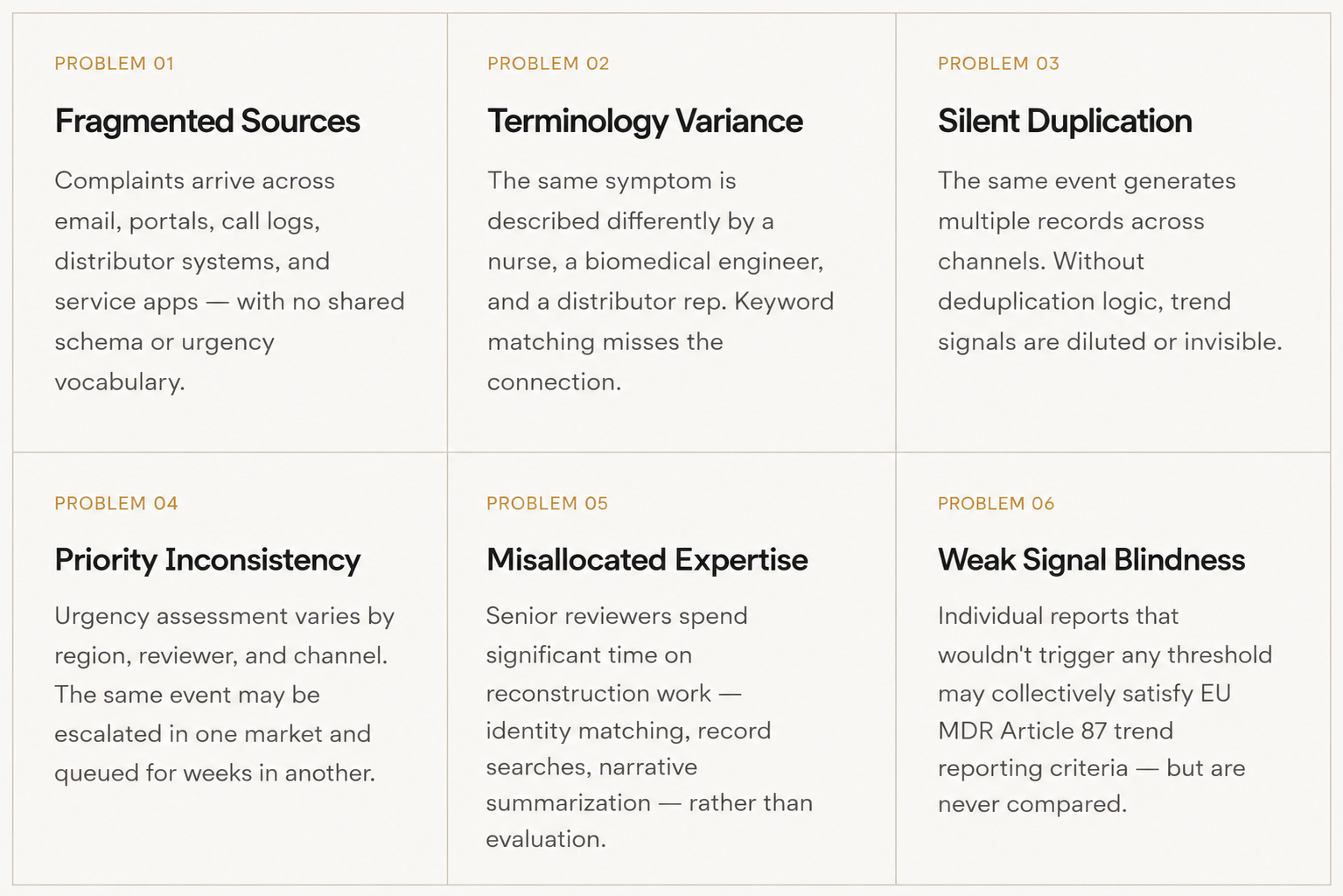
Complaints rarely arrive clean. They come through customer emails written in haste, call center summaries relayed second-hand, distributor messages filtered through commercial relationships, field technician notes using local shorthand, hospital communications in clinical terminology, and spreadsheets maintained outside any core system. Each source carries its own vocabulary, level of completeness, and threshold for urgency.
One report names a device family but omits the serial number. Another has the UDI but no symptom description. A third offers a detailed narrative using terminology no classification schema recognizes. One market codes an issue conservatively; another codes the same issue as a potential MDR-reportable event.
"Before judgment begins, someone must reconstruct identity, normalize language, compare narratives, search prior records, determine ownership, and decide urgency. By the time expert analysis starts, expert energy has already been spent on clerical interpretation." — RandomTrees Quality Intelligence
None of this is incompetence. It is the operational texture of any organization that has grown across geographies, product families, and commercial channels over time. But the consequence is real: trained reviewers routinely inherit not a case, but a puzzle.
Your QMS Stores Everything — But Answers Nothing in the Morning
The complaint management platforms used across the industry perform genuinely important functions. They preserve records, maintain timestamps, enforce access controls, route tasks, and support audit readiness. A controlled record is valuable. An auditable workflow is valuable. Structured documentation has real compliance significance.
But there is a meaningful difference between preserving information and clarifying it.
A system can store fifty thousand complaints and still struggle with the questions that matter at 9 AM on a Monday. Which open cases need attention today? Which incoming reports likely describe the same recurring event? Which product family is appearing more frequently than expected this quarter? Which queue is creating downstream investigation delays?
These are interpretation questions. Storage systems were not designed to answer them.
Historically, organizations addressed these problems through experienced reviewers who read widely, remembered patterns, and carried operational memory in their heads. That capability remains essential. But as portfolios expand and complaint volume grows, memory and manual comparison become less reliable forms of institutional intelligence.
The result is not organizational collapse — it is accumulating drag. Throughput variance increases. Queue times lengthen. Escalation decisions become inconsistent. And the people best equipped to assess seriousness spend measurable portions of their week performing work that should have arrived pre-organized.
Where AI Actually Belongs in This Process — And Where It Doesn't
Discussions about AI in regulated industries often collapse into two unhelpful positions. The first overpromises: AI will replace expert judgment and automate quality decisions. The second dismisses: regulated environments require human control, so meaningful AI use is impossible or too risky to pursue.
Both positions miss where practical value actually emerges.
"In regulated environments, the highest-value use of AI is not autonomous decision-making. It is the elimination of wasted motion around accountable decision-making."
— RandomTrees Quality Intelligence
The appropriate AI deployment in complaint handling is upstream of investigation — in the intake layer, where language must be organized, signals compared, records connected, and routine inconsistency reduced before qualified reviewers apply their judgment. That is a narrower scope than AI advocates often claim. It is also a more honest and defensible one.
None of these functions constitute a quality decision. They constitute preparation for one. The distinction matters both practically — for the quality team's efficiency — and regulatorily, since manufacturers must be able to demonstrate that trained, qualified personnel evaluated each complaint. AI that prepares information for that evaluation does not threaten that requirement. AI that claims to substitute for it does.
What Reviewers Actually Gain When Intake Gets Smarter
Efficiency claims in enterprise technology are almost always expressed in the abstract: productivity, throughput, transformation. Those terms obscure more than they reveal. Complaint operations offer more specific measures of what actually improves when intake quality rises.
The subtler gain — one that rarely appears in efficiency metrics — is the better allocation of institutional judgment. Organizations that deploy their most capable people to prepare information rather than evaluate it are not running a quality problem. They are running an operations problem. The distinction matters because the solution is different.
The MDCP Agent: Designed for This Specific Work
The MDCP Agent from RandomTrees — Medical Device Complaint Processing — was designed with this specific operational layer in mind. It is not a general-purpose assistant adapted to quality workflows. It was built for the intake stage: the period between complaint receipt and investigation start where information exists but coherence does not.
Its functional scope maps directly to the intake problems described above — classification consistency, record deduplication, narrative summarization, identifier surfacing, and early cluster detection. It is deployed through the RandomTrees AI Marketplace, which structures evaluation around specific functional work rather than general AI capability claims.
For quality teams evaluating AI in complaint operations, the right starting question is not whether AI is appropriate in regulated environments. It clearly is, within the right scope. The right question is whether the intake layer — the work before the work — is currently operating at the standard the rest of the process deserves.
"Serious complaints begin looking ordinary. That is not a technology problem. It is an information organization problem — and it has a tractable solution."
— RandomTrees Quality Intelligence
For manufacturers whose devices operate in clinical settings, complaint handling is part of the product experience, even when customers never see it. The moment a signal fails to consolidate, a duplicate goes undetected, or a weak cluster goes unnoticed is a moment where the system that should protect patients is running slower than it could.
Competent intake operations are not a luxury. For manufacturers subject to FDA, ISO 13485, and EU MDR obligations, they are an operational and ethical baseline.
References & Regulatory Basis
U.S. Food & Drug Administration. 21 CFR Part 820.198 — Complaint Files. Current Good Manufacturing Practice (CGMP) regulations for medical devices. ecfr.gov
U.S. Food & Drug Administration. 21 CFR Part 803 — Medical Device Reporting. MDR reporting timelines and manufacturer obligations. ecfr.gov
International Organization for Standardization. ISO 13485:2016 §8.2.2 — Complaint Handling. Medical devices — Quality management systems requirements for regulatory purposes.
European Parliament and Council. EU MDR 2017/745, Articles 87–89 — Serious Incident Reporting and Trend Reporting. Regulation on medical devices, May 2017.
FDA. Guidance for Industry and FDA Staff: Medical Device Reporting for Manufacturers. November 2016. fda.gov